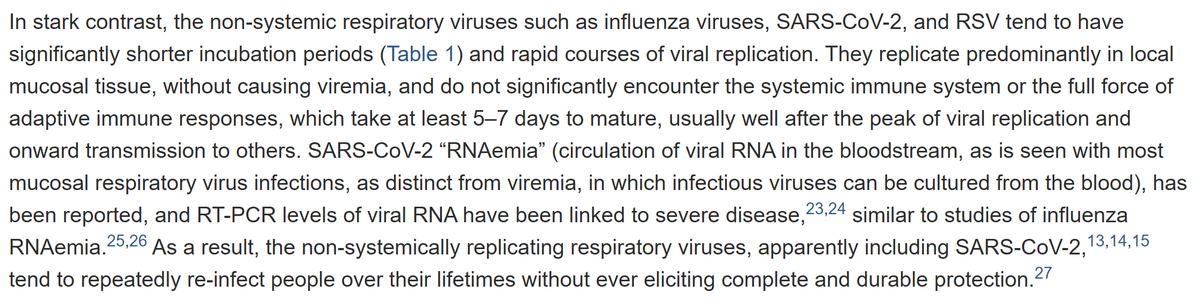
Dr Clare Craig
Mostly I agree with you on this John-but not 100%. Yes there was a virus and people died. Countries that had had no deaths pre-2022, all experienced excess mortality when covid did hit. However, unpicking deaths caused directly by the virus is tricky. The mortality rate was higher than for influenza if you include ALL covid labelled deaths. There are good reasons not to. One is overdiagnosis - PCR was detecting any incidental aerosol in the airway. When testing is done in the sick and dying this will create an illusion of a deadly virus. Furthermore, the total mortality in the worst waves was only as bad as previous bad flu seasons. Admittedly we hadn't had such a season fo 20 years - but the TOTAL mortality did not exceed deaths seen per capita prior to that period in bad years. The key is understanding that not all deaths are the same and not all covid labelled deaths were inevitable deaths. If you terrify care home staff and make 11% isolate simply because they have a cough - then you can expect mortality in care homes. The ones who tested positive will have a higher risk of dying (primarily from dehydration related issues) because staff believe their lives are at risk if they attend to them. Worse, end of life drugs were given to anyone not fit for intensive care on the basis that they were doomed. They were not doomed - even in the oldest groups and most frail, survival was substantially more likely than death. These drugs cause respiratory depression and lead rapidly to a viscious cycle of insufficient breathing, causing deterioration causing more drugs. People were given Do Not Resuscitate orders and depending on levels of covid in the hospital, hospitals refused to admit these people. The consequential death will therefore be highly correlated to the levels of tests positives in hospital at the time. If you stop giving people antibiotics for pneumonia (whether in a community or hospital) they will die more. This happened. These people tested positive. Yes, the virus was prothrombotic in a lab - but even Fauci admits it would only be as whole virus in blood (as opposed to RNA) in a handful of severe cases. See image. https://www.cell.com/cell-host-microbe/fulltext/S1931-3128(22)00572-8#%20 Other contributory factors to the clotting issues include stress. High cortisol levels increase clotting risk - and lockdowns and the fear of covid no doubt increased cortisol. People in hospitals with a covid label surrounded by masked staff would have had very high cortisol. From 2021, there was the added complication that the majority had been injected with a pro-thrombotic compound which definitely did enter the blood and not just in the tiny fraction of the population with a severe infection.